


























Arthrosis of the hip joint (coxarthrosis)- This is a chronic degenerative joint disease, leading to deformation of bone tissue.With coksartrosis, all components of the joints are involved in the pathological process: articular cartilage, bone structure adjacent to cartilage, synovial shell, ligaments, capsules and adjacent muscles.In the case of disease, the articular cartilage is destroyed, bone-micro-rentim and osteophytes (bone growth) appear, and inflammation of the muscles of the hip joint occurs.
In the world, every fifth person complains of problems with joints.This can be pain or restriction of movement in the joints, and the combination of these symptoms.Each second patient's vision falls in patients with bone muscle disorders, while 66 % of cases are people under the age of 65.According to the latest epidemiological research, the prevalence of arthrosis of the knee and hip joint in adult population is 13 %.
Risk Factors for Coxarthrosis Development:
- Genetic predisposition.The general cause of coksartrosis of the hip joint is a congenital mutation or a type of type II Prollagen.
- Old age.The cause of the possibility of arthrosis in old age is a contradiction between the damage to the cartilage along with the external environment and its ability to restore.
- Floor.Women have osteoarthritis more often than men.This is due to the effects of estrogen female sex hormone effects on bone-mineral metabolism.However, the influence of the floor is vague -samar - according to some authors, unlike damage to other joints, there is no difference in the sexual basis of coksartrosis: in men, hip joint arthrosis is as often found in women.
- Excessive weight.This relationship is proven between excessive body mass and arthrosis.Excessive adhesive tissue increases the damage to the cartilage.In addition, adipose tissue produces pro -inflammatory enzymes that damage cartilage tissue.
- Frequent development of bone and joints.In line with the study, 80 % of coxarthrosis, which occurs for no apparent reason, is associated with previous defects that are not diagnosed in the development of hip and sublasia.
- Heavy physical labor.Excessive load on the hip joint with certain types of physical labor can cause damage to the joints and the formation of arthrosis.At risk are agricultural workers, excavators and people with the same expertise.
- Injury.The risk of developing coxarthrosis increases after injury to the hip joint.In addition, both joints are injured and both may be involved in the process.
- Professional playing sports.Professional sports can trigger the occurrence of good coxarthrosis due to excessive burden on the joints and due to injury.Potential sports including heavy sports, sports jumps, parachute sports.
- Bone and joint disease- rheumatoid arthritis, psoriatic arthritis, joint infection, avascular necrosis, gouty arthritis, etc.
- Endocrine pathology- hypothyroidism, hypoparathyroidism, acromegali (impaired function of anterior pituitary gland), diabetes, obesity.
If the same symptoms are detected, consult your doctor.DON'T MAKE SURE - it's dangerous to your health!
Symptoms of arthrosis of the hip joint
The main symptoms of coxarthrosis include: pain, mobility restrictions and crisis in the joints, their deformation, functional shortening of lower limbs and regular swelling in the joints.
The pain of various intensity.The pain in the joints at first is not important and arises for a short time.They appear or intensify during walking or with other physical efforts, for example, during squats, tendencies and weight loss.As the disease develops, the pain increases and the long rest does not bring relief.In addition, pain occurs with prolonged immobility and joint fixation in one position.
Patients complain of "starting" pain in the hip joint after sleep, driving in the car and other prolonged immobility."Start" the pain for coxarthrosis lasts no more than 30 minutes.Pain is increasing during hypothermia or under stress.They can be localized in the back or thigh area, on the front or thigh surface.With the spread of pain on the lumbar plexus nerve, it can be transmitted to the thighs away from the center of the body or in the knee.Sometimes pain occurs in the lumbosacral and tailbone spine.

Co -operative mobility restrictions.Movement in the hip joint with coksartrosis is limited due to pain.At the same time, the rotation (turning inside and out) and carrying the lower limbs (movement to the center) is more often interrupted, but can be limited (movement from the middle axis), as well as flexion and extension.The inability to make passive movements in the joints due to significant pain syndrome causes the pelvic tendency to compensate.The change in the patient's gait, the back is attached, the body deviates forward when transferring weight to the damaged side.With bilateral damage in patients with coksartrosis, "duck gait" is formed.
With coxarthrosis occurs periodicallyswelling in the jointswhich can be seen because of the muscle and fat layers.Also, the disease is characteristicChrist in the joints during movement, their deformation gradually and the shortening of the lower limbs.
Often, one joint is affected by the disease, so the process applies to others.But sometimes arthrosis affects some joints at once and polyosostoarthritis occurs.Polyosteoarthrosis is a characteristic of the elderly or with the tendency of heredity and joint disease - bone disease, joints and endocrine disorders.
Pathogenesis arthrosis of the hip joint
In the pathogenesis of hip joint arthrosis, an important role is played by mechanical damage (injury and microtraumas due to physical improvement in the joints) and genetic, hormone and metabolic factors.It is usually not possible to know which factors affect the development of the disease in certain patients, but often the disease develops after tissue damage with mechanical injury.
Tissue damage stimulates cell division -cartilage tissue (condo), while the production of pro -inflammatory cytokine increases, which is usually found in cartilage only in small quantities.Cytokines launch the inflammation process, for example, under the influence of IL-1 pro-inflammatory cytokines, a distinguished enzyme that destroys the cartilage of the joints.Also, under the influence of cytokines, the production of TSOG-2 enzymes and other substances with toxic effects on cartilage increases.
Synovites also play a major role in the development of coxarthrosis - a synovial shell inflammation of the joints or ligaments with fluid accumulation in the cavity.
The decrease in elasticity and strength of the articular cartilage associated with metabolic disorders leads to its decrease in durability to mechanical stress.With coksartrosis, all components of the joints are involved in the pathological process, including the subcondral bone.Due to the fact that large joints of the lower lower leg contribute to large joints of the body, they experience significant mechanical stress, as microvaloma occurs in subcondral plates and cartilage.As a result of microveloma, the subcondral bone is compacted, leading to regional growth of bone tissue - osteophytes.And this, in turn, stimulates articular cartilage deterioration.
In some cases, hip joint arthrosis is inherited.Descent arthrosis is a polygenic legacy - due to the actions of many genes, each affecting weak.The cause of some diseases is a mutation in the genes of articular cartilage macromolecules, which cause rupture.The genes responsible for dividing chondrocytes may also suffer.In addition, metabolic disorders are inherited, such as pyrophosphate arthropathy - a disease in which calcium pyrophosphate crystals accumulate in articular cartilage and synovial fluid.
Classification and stage of development of hip joint arthrosis
Depending on the cause of the disease, coxarthrosis is divided into two main forms: main (idiopathic) and secondary (arising from or other diseases).
The main coksartrosis:
- Local (only hip joint affects):
- unilateral;
- two -way.
- General (polyosteoarthrosis) with at least three groups together (for example, hips, knees and small joints of brushes or feet).
Secondary arthrosis:
- Post -traumatic:
- Acute - due to acute injury;
- Chronic - due to classes of several sports or as a result of professional activities.
- Metabolic disease (oconosis, hemochromatosis, Wilson disease, gaucher disease).
- Congenital pathology and developmental defects (congenital displacement of hip joint, middle disease, slipped femur epiphyse, hypermobility syndrome, shortening lower limbs, scoliosis, bone displacement).
- Endocrine pathology (acromegali, hypothyroidism, diabetes mellitus, hyperparathyroidism, obesity).
- Calcium salt (arthropathy pyrophosphate, calcifying tendonitis).
- Bone and joint diseases (rheumatoid arthritis, psoriatic arthritis, pedhetic disease, avascular necrosis, infection).
According to clinical manifestations, the following forms of coxarthrosis are distinguished:
- A little sympic.
- Almost, indicated by bright clinical symptoms:
- rapid progressive, where symptoms develop in the first four years of the onset of the disease;
- Slowly progressive -Symptoms -Significant symptoms appear after five years of the disease.
In accordance with picture X -ray, two types of hip joint arthrosis can be identified:
- Hypertrophic - with signs of increased reparrative reactions (lesions are replaced by new tissues, for example, osteophytes appear);
- Atopic (decreased tissue volume).
The level of the disease can be determined by radiologically and clinically.To determine the radiological levels of hip joint arthrosis, the classification of Kellgren and Lawrence (1957) is most commonly used.
Stage of arthrosis in radiological classification
| Phase | Mark |
|---|---|
| 0 | There is no sign of arthrosis in image X -Ray |
| 1 | The joint gap does not change, a single regional osteophytes are described |
| 2 | The joint gap does not change, significant regional osteophytes |
| 3 | The height of the joint gap is reduced, significant regional osteophytes |
| 4 | The height of the joint gap is significantly reduced, significant regional osteophytes and subcondral osteosclerosis are visualized (compaction of bone tissue below the lower surface of the cartilage with cartilage structure) |
To determine the clinical stage of the disease, the classification (1961) was used, which used both clinical signs and visualization criteria.
Clinical stage of arthrosis
| Phase | Mark |
|---|---|
| 0 | The articular gap is narrowed indirectly and unevenly, the edge of the articular crack slightly pointed (early osteophytes), slight restrictions observed |
| 1 | The articular gap is very narrow (50-60 %), significant osteophytes, subcondral osteocosclerosis and cyst enlightenment in bone epiphyse;The clinic is dominated by mobility restrictions in joints, rough problems during movement, non -essential or moderate muscle atrophy |
| 2 | deformation, joint stiffness;The articular gap is narrowed by more than 60-70 % of the norm or absent, the broad osteophytes, subcondral cyst, the articular "mice" are visual bones, cartilage or mixed pathological formation located in the joint cavity |
Complications of hip joint arthrosis
With coxarthrosis, all complications are accurately associated with pathological changes in the joints.
Coksartrosis courses can be complicated by the local inflammation process:
- Bursite - inflammation of the synovial bag in the joints;
- tendovaginitis - inflammation of the internal skin of the vagina of the muscle tendon;
- Nerve-pinches-pinches syndrome due to large osteophytes formation or with joint deformation.
With the development of coxarthrosis and its transition to the clinical stages of II and III, pain limits joint movement, and over time, joint ankylosis (fibrous, bone or cartilage) occurs, accompanied by complete immobility.
Significant joint deformation can causeFracture or bone aseptic necrosis.For coksartrosis, femoral aseptic necrosis is the greatest complication.
With a clear coksartrosis, may occursubluxation and jointsas well as the penetration of the femoral head into the pelvic cavity.Dislocation and subluxation of the hip joint lead to pain (initially acute, then tedious and painful), intensified during walking and other physical work, as well as joint deformation, paralysis, and sometimes to shorten the affected member.
Despite the lack of systemic manifestations of arthrosis itself, in modern clinical practice, more attention is given to diseases associated with it.This is a pathological condition that exists or arises in the background of the current disease.In connection with the reaction of the inflammation arising during arthrosis, the formation of atherosclerotic plaque in the inner wall of the vessel is enhanced, which increases the riskCardiovascular disease.Decreased physical activity due to pain and mutual mobility restrictions leads toObesity, depression and deterioration in the quality of life.With the use of prolonged anti -non -—ssteroid drugs,The upper gastrointestinal part is affected,As well asThe risk of cardiovascular pathology and kidney disease increases.
Diagnosis of hip joint arthrosis
The diagnosis of "coksartrosis" is made based on clinical manifestations and radiological examination.There are no signs of laboratory features for arthrosis diagnosis.
Between clinical manifestationsThe main one for the diagnosis of hip joint arthrosis is its pain and character.Pain for arthrosis of the hip joint occurs and grows gradually for several years (sometimes a few months with a rapid progressive form).Pain occurs or increases during physical work or in standing position.If the patient starts to feel pain alone, then inflammation (synovitis) combines.The statement is recorded for up to 30 minutes in the morning and with prolonged immobility.
The boundaries of joint mobility gradually increase, this occurs for both active and passive movements.With the development of the disease, the joints are defective, the shortening of the functional limbs may occur.
At the physics examinationThere are joint mobility restrictions, their deformation, shortening the limbs, pain in joint palpation and large rotating from the femur, muscle atrophy.
Laboratory methodFor diagnosis of hip joint arthrosis is not required.However, they can be used for the diagnosis of differential coxarthrosis with arthritis (rheumatoid and chronic), as with arthrosis there is no change in inflammation in the whole blood test and rheumatoid factors, and uric acid levels do not increase.In addition, using laboratory tests, contraindications are lowered for drug treatment methods.
Instrumental methodFor diagnosis of hip joint arthrosis:
- Radiography- This is the main method for diagnosing arthrosis of the hip joint.Radiography determines the characteristics of the features of coksartrosis: narrowing the joint gap, osteophyte, erosion and cartilage ulcer, subcondral cyst and osteosclerosis.The X -ray examination is a classic method for diagnosis of coxarthrosis, and the radiological signs underlying the classification of coxarthrosis.However, at present, other methods of visualization of joints are increasingly used, such as ultrasound and magnetic resonance imaging.
- Ultrasound Examination (Ultrasound) -The advantage of ultrasound is without radial load on the body.
- Magnetic resonance tomography (MRI)- In comparison to other methods, it allows you to clearly describe joint damage.
- Arthroscopy-Allows you to identify damage to the articular cartilage: from the chondromation zone (softening the articular cartilage) with a diameter of less than 10 mm to the deep cracks that penetrate the subcondral bone and the formation of deep ulcers.Superficial and moderate fractures and surface erosion can also be described.
The identification of coksartrosis usually does not represent special difficulties, but when assessing certain clinical conditions, it is important to remember the original -the possible secondary arthrosis of the hip joint (as a complication of other diseases, for example, with endocrine disorders).
Treatment of hip joint arthrosis
Treatment of hip joint arthrosis can be conservative (medication and not constructed) or surgery.Conservative treatment is used at stage 1-2 diseases, 3-stage surgery.Surgical treatment can be recommended at 2 stages with persistent pain and lack of reactions to conservative therapy.
Conservative Therapy Goals:
- Improving quality of life - reducing pain and increasing joint mobility;
- Stop or slow down the development of the disease.
Non -Drug treatment methods include:
- Unloading the hip joint (weight loss, the creation of additional support and the transfer of weight to the cane or stick);
- Physiotherapy physical education;
- Physiotherapy treatment method.
Coxarthrosis treatment begins with a non -Drug method, an important role given to physiotherapy training.With severe pain, the patient should use support.With clear illness and the presence of contraindications to endoprostetics, support should be used for life.
Cuxartrosis drug therapyIncludes medications that reduce the symptoms of the disease.These are analgesics, as well as drugs from the anti -non -ssteroid drug group (NSAIDs).NSAIDs are divided into selection and selective.
Analgesic and NSAIDs for hip joint arthrosis are used for a short time to relieve pain and inflammation.Currently, there is no proven advantage of one non -stable anti -agent on the other, so certain drug choices depend on the specific side effects and clinical conditions caused by it.
Keep in mind that NSAIDs have some side effects.When taking it, the mucous membranes of the stomach and duodenum are affected, resulting in ulcers and bleeding.A number of NSAIDs have toxic effects on the liver and kidneys.In addition, NSAIDs disrupts platelet aggregation, and, as a result, the patient is disrupted by thrombosis and there is a tendency to bleeding.NSAIDs with prolonged use suppress the hematopoiesis process and can cause aplastic anemia and agranulocytosis.Selective NSAID acceptance causes less complications.
Located ointments and gels cause less side effects from oral products.For the treatment of arthrosis, medications with heating and reducing pain are used.They can contain turpentine, bulbs, nicotinic acid esters, salicylates, bees.Also, NSAIDs have a good effect.
In the absence of analgesic and NSAIDs effects or if it is not possible to choose the optimal dose of the drug, the central action painkillers can be prescribed short.
In the case of inflammation, intra -articular administration of corticosteroids is used.Corticosteroids are used no more than 2-3 times a year, as more frequent use can cause cartilage degeneration.
Slowly acting drugs weakening the symptoms of the disease including chondroprotectors, an inappropriate compound of avocado or soy, hyaluronic acid.These drugs are included in the European Antirematic League recommendations for the treatment of hip joint arthrosis.Preparation reduces pain and increases mobility together.
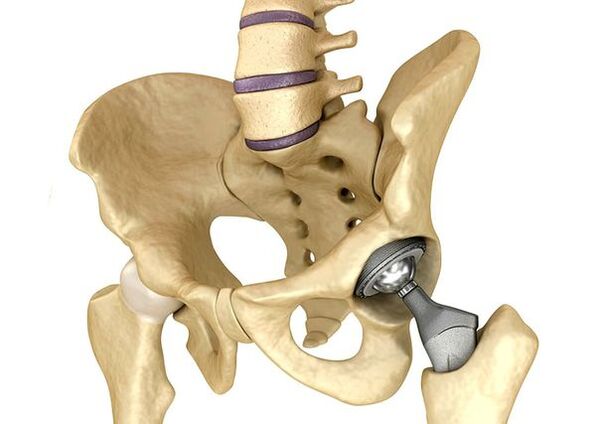
Endoprostetic hip jointIt is used in cases of severe stage III, when the pain syndrome cannot be eliminated, and the movement of the joints is limited.Prosthetic hip joint leads to a decrease in pain syndrome, improving the functional condition of the joints and the quality of life of the patient.The effect persists for 10-15 years, after which the second operation may be needed.During surgery, the hip joint is replaced by a ceramic, metal (most commonly used titanium prostheses) or polymer.
Forecasts.Prevention
The prognosis of hip joint arthrosis in relation to the patient's life is good, but the disease often causes defects.According to the World Health Organization, 80 % of older patients with coxarthrosis have mobility violations, and 25 % cannot do things daily.In this case, the main prevention of hip joint arthrosis is important.
Preventive measures:

- Lose weight.It needs to adjust the nutrition to lose weight and the burden on the joints.In addition, a decrease in the amount of adipose tissue reduces the amount of inflammation mediator released.
- Avoid heavy physical labor and too much sports.Physical load often causes arthrosis of the hip joint, while moderate physical activity, in turn, improves the articular cartilage, maintains its normal mobility and reduces the burden on other joints.
- Correct the underlying disease.If the patient is detected in a disease that can cause secondary coksartrosis (endocrine, rheumatism and other), underlying disease is required.Normalization of hormone background and continuous remission of rheumatic disease is a major prevention of arthrosis, and allows you to slow down its development.
- Lead a healthy lifestyle.A diet that is balanced with adequate plant and animal protein content, unsaturated fatty acids and limits simple carbohydrates, as well as moderate physical activity, avoiding coxarthrosis even in the face of risk factors.
Currently, prevention of hip disease is mandatory in neonatology and pediatrics.At the same time, congenital displacements coordinated with the hip joint significantly reduced the risk of coxarthrosis in adulthood.